Research
The general goal of our research is to assess the function of brain structures such as the amygdala, medial prefrontal cortex, and hippocampus in PTSD. Our research suggests that the amygdala and dorsal anterior cingulate cortex are hyper-responsive while the ventral medial prefrontal cortex is hypo-responsive in individuals with this disorder.
The lab currently conducting studies to determine (1) whether functional brain abnormalities in PTSD are acquired signs of the disorder or familial vulnerability factors that increase the likelihood of PTSD after trauma exposure and (2) whether these functional neuroimaging measures can predict response to treatment.
Current Research Questions
What is the Origin of Functional Brain Abnormalities in PTSD?
PTSD is a relatively recent addition to the psychiatric diagnostic system used in the United States, and researchers have only just begun to investigate the biological bases of this disorder. In order to determine whether the functional brain abnormalities in PTSD are acquired characteristics of the disorder or familial vulnerability factors for its development, we are conducting fMRI studies of amygdala, medial prefrontal cortex, and hippocampal function in identical twin pairs. Within each pair, one individual served in Vietnam and the other twin did not. In half of the pairs, the combat-exposed twin has PTSD; in the other half, the combat-exposed twin does not have PTSD (see figure below).
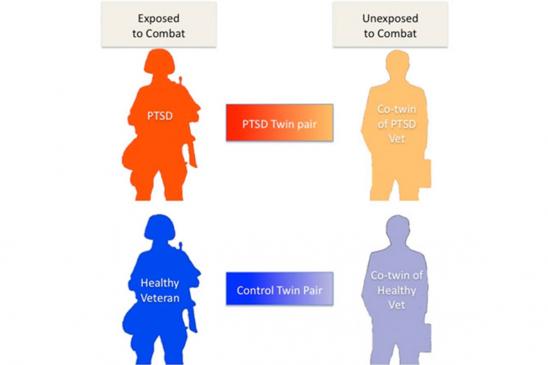
Twins participating in the study perform a variety of tasks in the fMRI scanner while brain activation is measured. If a specific functional brain abnormality is found only in the combat-exposed participants with PTSD, that would suggest that the abnormality reflects an acquired characteristic of the disorder. If a functional abnormality is found in both the combat-exposed participants with PTSD and their combat-unexposed identical co-twins without PTSD, that would suggest that the abnormality reflects a familial vulnerability factor. If a functional abnormality is observed in the combat-exposed veterans both with and without PTSD and not in their combat-unexposed identical co-twins, that would suggest that the abnormality is associated with trauma exposure (and not PTSD). Evidence thus far suggests that hypermetabolism and hyperactivity of the dorsal anterior cingulate cortex may be familial vulnerability factors, whereas other measures (e.g., heart rate responses to loud tones) are acquired signs of the disorder.
Within the twin design, we are also studying brain structure, white matter tracts, and the relative concentrations of metabolites in the brain, such as N-acetyl aspartate. Additionally, we are examining glucocorticoid stress hormone receptors within blood cells in order to determine why individuals with PTSD may be more sensitive to the effects of the stress hormone cortisol.
In the future, we hope to expand this line of research to include twin veterans of more recent military conflicts, such as Operation Enduring Freedom and Operation Iraqi Freedom.
Can Neuroimaging Measures Predict Treatment Response?
This line of research seeks to determine whether pre-treatment neuroimaging measures of amygdala and medial prefrontal cortex function can predict response to treatment with behavioral therapy in PTSD. Preliminary findings show that higher pre-treatment activation of the ventral medial prefrontal cortex and lower pre-treatment activation of the amygdala in response to predictors of potential threat (i.e., fearful facial expressions) are associated with greater symptomatic improvement following behavior therapy.